[vc_row][vc_column width=”2/3″][vc_column_text]
Narrowing the Language Gap in Medical Tourism: Communications Guidelines for Physicians
Part 4: Practical “Tips” for Improving Clearer Patient Communication
- Arrange for a trained and certified[1] medical interpreter to be available regardless of how well you speak the patient’s language or how well you think he/she speaks yours, prior to the patient’s scheduled visit. If you feel comfortable speaking that the patient’s language you might conduct the visit in that language, but, unless you have been certified by a medical language specialist in your fluency in the patient’s language, ask the patient’s permission for an interpreter to be present[2].
- Speak slowly, not loudly. Remember: The patient is hard of understanding and not hearing! A loud voice may intimidate the patient because it can be interpreted as anger or impatience.
- Use short, simple sentences. If you are conducting the exam in the patient’s language, don’t try to demonstrate your knowledge of that language by using idioms or colloquial words or expressions as you may use them incorrectly. If you are conducting it in your language, help the patient (and the interpreter!) understand your meaning by keeping it “short and simple.” Be pleasant, but avoid jokes or attempts to elaborate with examples, asides, or additional information which might “cloud” meaning in either your or the patient’s language
- Check understanding often by asking the patient to tell you in his own words, what you have said. Repeat what you have said using other words often. Check your understanding of what the patient has said whether the exam is being conducted in your language or in his. You might use expressions like, “So you have told me that the pain usually occurs in the evening. About what time (or after what activity) does it usually occur?
- Refrain from asking questions that can be answered by, “yes” or “no”—especially avoid the questions, “Do you understand?” or “Do you Agree:? A nod of the head or a “yes” may only mean that the patient has heard you, not that he understands or agrees to follow instructions. Use questions beginning with words like: what, where, why, when, how because they require answers that carry informatio
- If you are using an interpreter, make sure you give him “thought time” to give you the most accurate translation. Also keep in mind that it may take more words/time in either the patient’s language or your own, to convey the same meaning
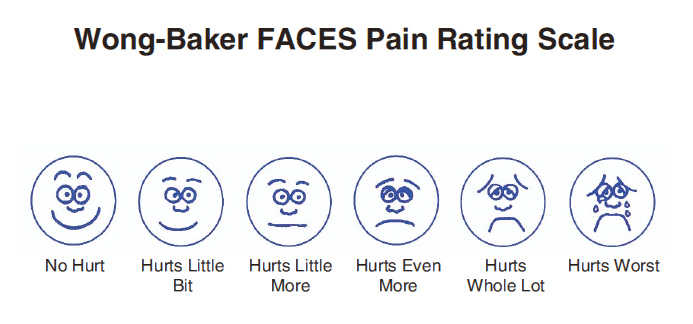
- Use as many visuals as possible. For example, a pictorial pain scale is helpful.
- Make sure that all patient instructions are in the patient’s native language. When prescribing a medication that the patient will fill in a pharmacy in your country, give the patient written instructions in his native language that tell him how to use it.
- If you send the patient somewhere else for tests or labs, make sure that the patient’s instructions regarding where to go, who to speak to, and what will be done are in his language and in writing. However, also give the patient written instructions to hand to that department or office explaining why you are sending the patient to that office and what services or tests are to be done.
- At the end of the visit, ask the patient to summarize your conclusions, the medical plan, what he must do next. This is often referred to as the “teach back” technique to test a patient’s understanding and willingness to follow instructions. In addition, give a written summary of conclusions and instructions regarding his/her next steps in the patient’s language in case any information is forgotten after leaving your office. Ask whether he or she has any further questions or whether there is any information which he/she would like the interpreter to translate.
[1] Although, there is yet not globally recognized body which certifies medical interpreters, there are well-reputed public and private medical interpreter training programs in many countries. Most require a minimum of 40 hours of training and issue a certificate upon completion.
[2] Off-site interpreters available via phone or video might be an option in some countries.
[/vc_column_text][/vc_column][vc_column width=”1/3″][vc_column_text]This article is part of a series by Dr. Suzanne Salimbene, a senior consultant with the Mercury Advisory Group. Dr Salimbene’s book, What Langauge Does Your Patient Hurt In? is currently being revised for 3rd edition release later this year.
[/vc_column_text][vc_column_text]
Learn more about culturally Competent Care with the US Department of Health and Human Services Office of Minority Health.
In April 2013, the National CLAS Standards were re-released after undergoing a two-year enhancement initiative. This program, along with others featured on TCH, is scheduled to be under annual review for accreditation purposes and will be updated to reflect the National CLAS Standards enhancements.
To assist you during this transition, we recommend that you reference this crosswalk (PDF – 115 KB) and fact sheet (PDF – 59 KB) which will assist in understanding the numbering and organization of the re-released National CLAS Standards.[/vc_column_text][/vc_column][/vc_row]
